PROLAPSE
WHAT IS A PROLAPSE?
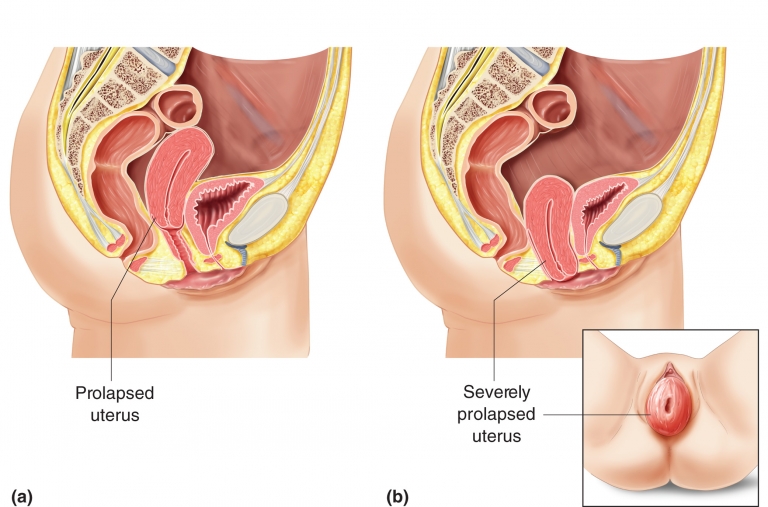
Prolapse of the uterus or the vaginal walls, out of the vaginal opening, is called genital prolapse. It is similar to a hernia, because the weakness of the supporting tissues/pelvic floor muscles allows the prolapse to come down into the vaginal opening. There are three main types of prolapse. First is the prolapse of the uterus, shown below;
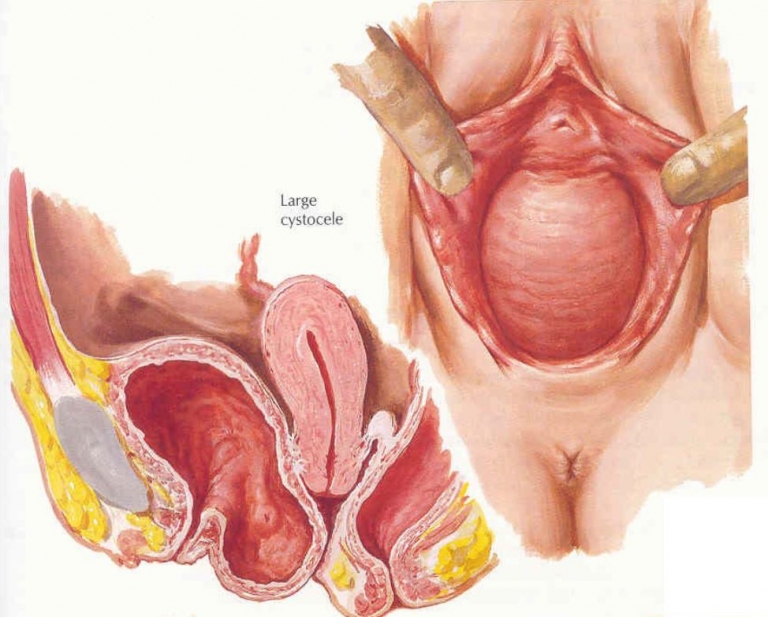
The second type of prolapse is prolapse of the bladder, shown below
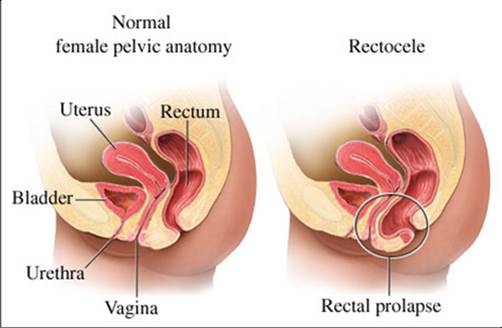
The third type of prolapse is prolapse of the rectum into the vagina, as shown below
WHY DOES A PROLAPSE HAPPEN?
Similar to hernia, a prolapse often occurs when the supporting tissues/pelvic floor muscles cannot cope with increased pressure down onto the vaginal opening. Common causes of increased pressure in the abdomen that cause genital prolapse are:
Obesity: No one wants to be as skinny as a rake, but if you are more than 15-20% overweight, the fat inside your body presses on the pelvic muscles and bladder. Inside your abdomen, there is a lacy apron coming off your bowel. It is called the omentum. In a thin person it is like fine lace. In an overweight person, the bottom of the apron develops fat pockets, for storage of excess fat. These press on the pelvic floor and bladder, making it much harder for the pelvic muscles to support the bladder when you cough.
Chronic Cough: With all this talk about coughing putting a stress on the pelvic floor, you can imagine how important it is to get rid of any chronic cough. If you have sinus trouble, with post nasal dripping of mucus, we will ask your doctor to refer you to an ear, nose and throat surgeon. If you have smoking related cough or bronchitis, stopping smoking will help your bladder to stop leaking. If you have asthma, seeing your doctor or a specialist respiratory physician may help by improving your asthma control.
Constipation or straining to open the bowels: If you have to strain to pass your bowel motion, because it is too hard, then every time you strain down to empty the bowel you are straining on your pelvic floor muscle. This weakens it and makes incontinence or prolapse worse.
How do I cure constipation?
Firstly, try to drink an adequate amount of water or other non-caffeinated fluids every day. The recommended amount is 2 litres every day. Many people with prolapse or incontinence cut down on their fluids to prevent frequent toileting. But if they get constipation, it worsens the prolapse or incontinence and so creates a vicious cycle.
Can I take a laxative to help?
Yes, you can take Metamucil, but only a small teaspoon in a large glass of water daily. This is because Metamucil works by drawing the water into the particles and making the bowel motions softer, or more full of water. Other similar medicines are Psyllium husks or Movicol Studies have shown that long term taking of Senokot tablets are harmful, because they only act on the nerves in the lining of the bowel, making it try to compress or squeeze the bowel contents more vigorously out the bottom end. Eventually the nerves get tired and the Senokot doesn’t work as well, so the person needs more of it to get the same effect. We do not recommend Senokot! Sometimes stool lubricating medicines such as Lactulose or Aqacol may give additional help.
Chronic heavy lifting, eg heavy gardening, or carers who lift disabled relatives in/out of bed: These can cause raised abdominal pressure that is transmitted to the vagina and it is very important that this should be corrected as part of the treatment of prolapse. Having said that, it is very rare to see prolapse in women who have no children. As you can imagine, carrying the extra weight of a pregnancy in the abdomen for 40 weeks causes considerable strain on the pelvic floor muscles but since only about 20% of all women seek help for prolapse, childbirth is not “the cause”. Age has an important effect, probably reflecting the beginning of Menopause.
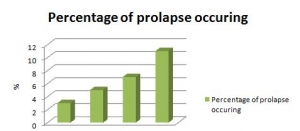 Prolapse occurs in
Prolapse occurs in
- 3% of women aged 40-49
- 5% of women aged 50-59
- 7% of women aged 60-69
- and 11% of women aged 70-79.
As you can see, it is probably the combined effects of menopause, increasing age, against a background of previous childbirth, with obesity, chronic cough, constipation, heavy lifting, or a combination of these, acting as “the final straw”.
WHAT ARE THE TREATMENTS FOR PROLAPSE?
The treatment options for prolapse include:
- Correction of the above risk factors such as obesity, chronic cough, constipation
- Referral to a pelvic floor physiotherapist for pelvic floor muscle training
- Vaginal ring pessaries
- Surgical operations
Expert Physiotherapy
If you are having trouble performing your pelvic floor exercising programme on your own, studies have shown that visiting a specially trained pelvic floor physiotherapist will help. This type of physiotherapist has taken a special post-graduate course of instructions on how to treat stress incontinence. She will see you weekly or fortnightly for up to 12 weeks. She will check the strength of your pelvic floor muscle, and gradually increase your pelvic floor exercising programme, a bit like a “personal trainer” in the gymnasium. She will teach you how to perform short, sharp squeezes of the muscle, along with longer, sustained squeezes, in specific patterns throughout your day.
Vaginal ring pessaries
Vaginal ring pessaries are plastic or silastic devices specially shaped to fit in the vagina and elevate the prolapse. They are especially useful for women who are not fit for surgery or who have not completed their family. There are different shapes and sizes. They are inserted by a doctor/nurse and only kept if they are comfortable. These need to be changed every 4-6 months by a nurse, or many patients can remove and wash them monthly, then see the doctor annually.
Surgery
Most commonly, a vaginal repair operation is performed to correct vaginal prolapse. In severe cases, an abdominal operation may be needed to correct the prolapse, which may be performed by keyhole surgery or open abdominal operation. There are different types of prolapse, so each patient needs to discuss individual details with the doctor concerned.
FURTHER READING
Patient Information Leaflets (click on a link below to download information). The following resources have been provided by the UroGynaecological Society of Australasia and are intended to be used as a guide for information of general nature.